
Written by: Kane York
Editors: Sophie Hill, Austin Shannon, and Peijin Han
I’m running low on serotonin
Chemical imbalance got me twisting things
Stabilize with medicine
There’s no depth to these feelings
-“Serotonin”, girl in red
Depression. In the time of a global pandemic, a burning ocean, an increasing wealth gap, and other catastrophes too numerous to mention, what could be more topical? Depression is one of the most common illnesses in the world, affecting more than 322 million people. Despite its prevalence, depression is still not perfectly understood. The common view is that depression is caused by an imbalance of chemicals in the brain, but the current research tells us that the condition is far more complex.
What is Depression?
There are several types of depression. The Diagnostic and Statistical Manual of Mental Disorders (5th edition), the primary guidebook that professionals use to diagnose mental illnesses, defines depression by the criteria listed below. To be diagnosed with depression, a person must have a depressed mood or loss of pleasure and meet five of the below criteria for at least two weeks.
- Depressed mood
- Decreased interest or pleasure in almost all activities
- Appetite or weight disturbance
- Sleeping more or less than usual
- Slowing of thoughts or physical movements
- Fatigue
- Feelings of worthlessness
- Diminished ability to think or concentrate
- Repeated thoughts of death and suicide
This list is primarily concerned with “Major Depressive Disorder (MDD).” This is usually the condition that most people have in mind when thinking about depression, but it is not the only form of the disease. Others include:
- Persistent Depressive Disorder (PDD), formerly known as dysthymia, includes most of the criteria for Major Depressive Disorder but lasts for at least two years. It is usually not as severe, but the symptoms are long-lasting.
- Bipolar Disorder, a type of depression that is defined by episodes of mania and depression. Manic episodes are characterized by a grandiose sense of self, extreme level of self-esteem, and little need of sleep, while depressive episodes are similar to other types of depression.
- Seasonal Affective Disorder has all the hallmarks of MDD but is brought about by climate conditions (sunlight, weather, etc.). Depressive symptoms usually occur during the winter but can also be observed during the summer.
- Perinatal Depression is characterized by the typical depressive symptoms with the exception that they are linked to a pregnancy—either during the actual period of pregnancy or up to 12 months after.
- Premenstrual Dysphoric Disorder (PMDD) is depression associated with premenstrual syndrome that usually begins after ovulation and ends once menstruation begins.
Is depression really just an imbalance of chemicals?
The causes of depression are as varied as the disease itself. There is a pervasive idea that depression (and other mental illnesses) can be reduced to an imbalance of certain brain chemicals, known as the Chemical Imbalance Theory. This idea is so widespread, in fact, that it’s present in television shows, songs (see the lyrics at the beginning of the article), internet memes, and more. The theory is simple: depression = low amounts of [insert neurotransmitter here].
Neurotransmitters are chemicals that brain cells (neurons) use to communicate. One neuron releases neurotransmitters that bind to receptors on a neighboring neuron. This binding causes the second neuron to either activate (turn on) or deactivate (turn off), which determines whether it sends a signal to other neurons or not. In the case of depression, the neurotransmitter in question is primarily serotonin, which affects mood, appetite, and sleep.
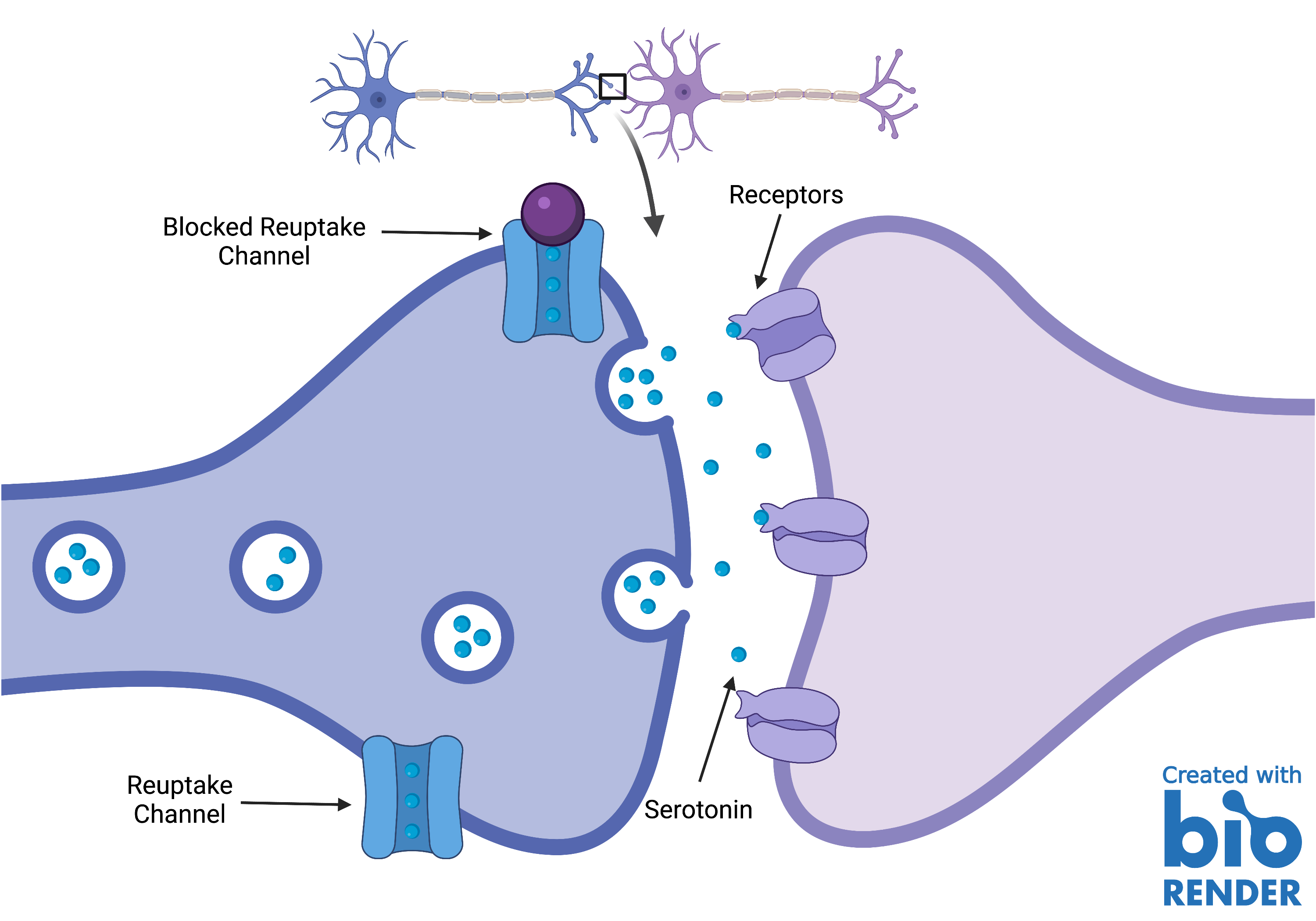
To treat depression, physicians generally prescribe medications called Selective Serotonin Reuptake Inhibitors, commonly known as SSRIs. Typically, after a neurotransmitter has been released and binds to a receptor of another neuron, the neuron that released the neurotransmitter reabsorbs “leftover” neurotransmitters via reuptake channels. SSRIs block these channels, allowing the serotonin to spend more time in the gap between both neurons, and thus, binding to the receptors more often (Fig. 1).
So, increase the amount of serotonin → decrease the depression, right? If only it were that simple. To its credit, the Chemical Imbalance Theory is partially true; SSRIs do decrease depressive symptoms. However, there is more to depression than a lack of serotonin. First, even though SSRIs increase the concentration of serotonin shortly after ingestion, it can take weeks for one to feel the effects of the medication, suggesting that a lack of serotonin is not the whole story. Second, SSRIs do not work for everyone. Some people only feel partially better while some feel no effect at all. Third, there are other neurotransmitters implicated in depression (e.g., dopamine and norepinephrine).
Even the scientist who proposed Chemical Imbalance Theory in 1965 stated that the model was reductionist and overly simplified. There are many other factors—biological and environmental—that can be linked to depression. One of these is the size of certain brain regions. Specifically, scientists find structural differences in the brains of patients with depression. One area of interest is the hippocampus, a seahorse-shaped brain region that is important for memory. Several studies have found that depressive episodes are correlated with decreased hippocampal mass. Some studies have proposed that the life stresses that often lead to depression are the cause of these abnormal sizes. These stressors lead to the difficulty of creating new neurons in the hippocampus, and thus, the hippocampus is smaller. Interestingly, antidepressants have been shown to increase the development of new neurons in the hippocampus. This could be a possible explanation for why it takes weeks for patients to feel the effects of antidepressants. These studies are still in progress and a definitive conclusion has not yet been reached concerning this possible connection.
Inflammation may also have a role to play in depression. Inflammation is part of how the body protects against damage and infection. Patients with major depression have increased levels of cytokines, molecules that are released from cells during inflammatory responses. Importantly, numerous cytokines have effects on the key neurological sites for depressive symptoms. Examples of these depressive symptoms include anhedonia (inability to feel pleasure), increased sensitivity to negative experiences, and suicide.
Another factor is genetics. The information in every cell of your body has an inseparable role in your development, including the development of the brain. There are twin studies that suggest the genetic involvement in depression is around 50%. In other words, 50% of the potential causes of depression can be linked to one’s genes. Now, this is not to say that there is a “depression gene.” It is rare to make a one-to-one connection between a disorder and a gene. It is more likely that a gene or several genes interact with the environment and ultimately result in the symptoms of depression. The question of what gene(s) is still open though. A 2018 report found 44 genes implicated in the development of MDD. In short, we are far from establishing a simple connection between the onset of depression and the number of the factors implicated in its emergence.
The Complex Road from Physiology to Psychology
I have only scratched the surface of what scientists have uncovered and are currently researching with respect to the causes and treatment of depression. Additionally, most of what I have discussed is research regarding depression in general or MDD. More still needs to be done to address the specifics of the other types listed above.
Unfortunately, there is not a clear-cut answer for depression. The Chemical Imbalance Theory provides some clarity, but it is far from the full picture. Brain size differences, inflammation, and genes are just a few from the list of factors implicated in the development of depression. The connection between our physiology and psychology is a complex problem, and the theories presented here are a part of a broader effort to understand and treat enigmatic illnesses like depression. I hate to be the one to correct “girl in red”, but chances are that a low amount of serotonin isn’t the only reason her mind has “got [her] twisting things.”

A. Kane York is a Neuroscience Ph.D. candidate in Dr. Giancarlo Vanini’s lab, where he studies the neural circuitry of sleep. When he’s not in the lab, Kane occupies his time with video games, non-fiction books, and D&D. Kane is dedicated to science communication and hopes to show that science is one of the best endeavors humans have embarked upon.

One thought on “Depression: Physiology to Psychology is Rarely Simple”