
Written by: Madison Fitzgerald
Edited by: Ryan Schildcrout, Jennifer Baker, Christina Del Greco, Ari Hoffman, and Emma Milligan
Illustrated by: Zoe Yeoh
We inherit a lot of things from our parents–an old jean jacket, family recipes, or even a penchant for dessert. On the cellular level, we inherit a set of genes from each of our parents that determine traits like eye color and blood type. In some unfortunate cases, people can inherit genes that cause disease. Most treatments that are currently available for genetic diseases help manage symptoms but are not curative because the disease-causing gene remains broken.
What if we could fix these bad copies of genes? For the first time, the Food & Drug Advisory (FDA) has approved a therapeutic that uses new gene editing technology from bacteria to do just that. This technology is based on our understanding of CRISPR, a type of bacterial immune system. CRISPR systems are composed of repetitive regions of DNA that are interspersed with DNA from the genomes of bacterial viruses. These sections of viral DNA enable CRISPR to act like a vaccine for bacteria. In humans, vaccines help our bodies remember what a pathogen “looks like,” enabling a rapid immune response. In bacteria, saved viral DNA allows CRISPR to “remember” viruses from previous infections. When the same virus tries to infect the bacterium again, CRISPR machinery specifically targets this virus’s DNA to prevent the virus from replicating. In 2012—25 years after CRISPR was first observed and 7 years after its function as a bacterial immune response was discovered—scientists determined that they could give any DNA fragment to the CRISPR machinery, enabling the use of CRISPR for gene editing. This discovery had incredible potential for both basic research and therapeutics and won the Nobel Prize in Chemistry in 2020.
Fast forward to 2023, and scientists have successfully engineered CRISPR to cut and edit a specific piece of DNA in human cells to cure sickle cell disease (SCD). This rare genetic disorder results in defective adult hemoglobin, the protein that shuttles oxygen from your lungs to the rest of your body. In people with SCD, damaged hemoglobin causes their red blood cells to stick together more easily, which can cause severe pain and organ damage, and elevates the risk of infection and stroke. SCD patients currently receive therapeutics such as hydroxyurea aimed at alleviating symptoms, preventing complications, and reducing pain. Young SCD patients with minimal organ damage may receive curative bone marrow transplants, but this carries its own risks and requires a closely matched donor. Now, CRISPR-based gene therapeutics provide a potentially lifelong cure for SCD patients.
A gene therapy for SCD was made possible by decades of basic science research. In 1886—a century before the discovery of CRISPR—scientists discovered that our body makes two types of hemoglobin: fetal hemoglobin and adult hemoglobin. Fetal hemoglobin binds more tightly to oxygen, ensuring that fetuses can outcompete the mother’s adult hemoglobin to acquire oxygen in utero. After birth, a gene called BCL11A tells your red blood cells to stop making fetal hemoglobin and start making adult hemoglobin. However, production of fetal hemoglobin does not completely go away in adults. In 1948, scientist Jane Watson observed that SCD patients that retained higher levels of fetal hemoglobin production experienced milder symptoms. This was an important clue for developing SCD therapeutics; perhaps resuming fetal hemoglobin production could alleviate symptoms of SCD. However, completely turning off BCL11A would disrupt important processes in other types of cells, so scientists would need to turn off this gene in red blood cells only. The final piece of the puzzle was the discovery of a short DNA sequence that specifically tells red blood cells to turn on BCL11A. Editing this piece of DNA would turn off BCL11A exclusively in red blood cells, allowing this gene to remain active in other types of cells. With this approach in mind, Vertex Pharmaceuticals leveraged decades of basic science research to develop CRISPR-based therapeutic called Casgevy to cure patients with SCD.
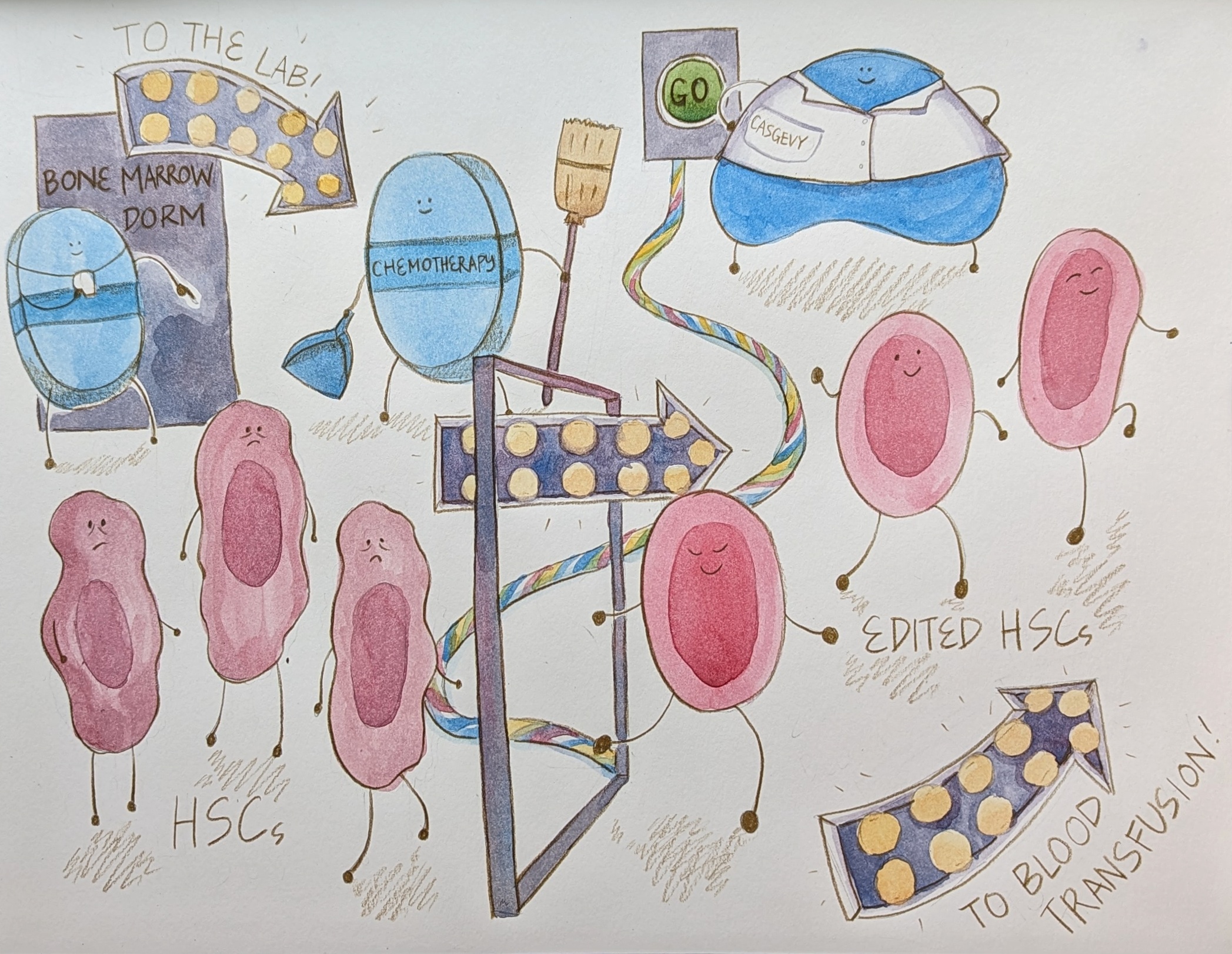
Armed with gene editing technology from bacteria and a genetic target for SCD treatment, researchers next needed to determine how to deliver a CRISPR-based therapeutic to red blood cells. Thankfully, they could adapt existing medical protocols for bone marrow transplants, which are used to treat blood disorders and cancers. The bone marrow is home to hematopoietic stem cells (HSCs), which develop into all the different types of blood cells. By targeting HSCs, Casgevy can specifically edit the DNA of cells that will develop into red blood cells. To isolate HSCs, the patient is given a drug that tells these cells to move out of the bone marrow and into the blood. After collecting HSCs from the blood, these stem cells are edited by Casgevy in a laboratory to activate the production of fetal hemoglobin. Before the edited HSCs can be returned to the patient’s body, the patient receives a chemotherapy drug which will kill the HSCs that remain in the bone marrow. This step is required to enable the new HSCs to establish in the patient’s bone marrow. Next, the edited cells are returned to the patient through a blood transfusion. During this time, patients can get sick more easily and are closely monitored by doctors to ensure their HSCs start developing into blood cells.
During the clinical trial process, Vertex Pharmaceuticals focused on measuring its ability to reduce vaso-occlusive crises (VOCs), which are when the sickled red blood cells form clumps that severely restrict blood flow and prevent parts of the body from receiving enough oxygen. VOCs are a major symptom of SCD and can result in organ damage. A global study found that the surveyed SCD patients experienced an average of 3 VOCs in the last 12 months, and 39% of respondents experienced at least 5 VOCs during this period. In the Casgevy clinical trial, 93.5% of patients who received the therapy experienced no VOCs in the twelve months following transfusion. The median number of VOC-free months after receiving Casgevy was 22.2 months.
Further work is required to determine if Casgevy can provide decades of protection against VOCs and alleviate other symptoms of SCD, and an ongoing long-term follow-up study aims to address some of these questions. Vertex is also investigating whether Casgevy is safe for kids and if it can cure other blood disorders. Still, widespread administration of Casgevy faces several logistical hurdles. Collection of HSCs and administration of chemotherapy require specialized healthcare infrastructure and expertise that is not present at every hospital. These therapies are also quite expensive–Casgevy costs $2.2 million per patient. A 2023 study estimated that SCD patients accumulate $1.7 million in healthcare costs during the first 64 years of life. Combined with quality-of-life improvements such as alleviating chronic pain and reducing the risk of stroke and infection, Casgevy could prove cost-effective if these treatments are indeed curative.
The FDA approval of Casgevy represents a major step forward for people living with SCD. While SCD is not a common disease, there are 100,000 Americans whose lives could be improved by this treatment. Living SCD-free would mean less fatigue, fewer hospital visits, and the ability to exercise and travel to high altitudes without fear. SCD disproportionately affects Black and Hispanic Americans, so Casgevy is a rare example of pharmaceutical companies prioritizing therapies to improve the health of people of color.
Casgevy is also the first FDA-approved therapy that leverages CRISPR, a relatively new gene editing technology that shows great promise. There are only 34 FDA-approved cellular and gene therapy products, and 8 of these are cord blood banks that facilitate bone marrow transplants. One challenge in developing gene therapies is identifying a therapeutic target that is specific and does not affect other biological processes. Additionally, delivering gene therapies to specific cell types continues to be difficult. SCD was a perfect proving ground for CRISPR-based therapies because these two challenges were easily surmountable—scientists had already found the target and had a method to specifically isolate HSCs. However, other genetic disorders will require further research to identify the genetic drivers of disease and develop new tools to target specific cell types. FDA approval of Casgevy is an important milestone in the field of personalized medicine and adds a new gene editing technology to our pharmaceutical toolbox. As this toolbox grows, so will our ability to develop curative therapies for genetic diseases like SCD.

Madison Fitzgerald is a sixth year Ph.D. student in the Microbiology & Immunology department. Her research focuses on gene regulation in a bacterium that causes catheter-associated urinary tract infections.
